
What is behavioural science?
And why is it essential in planning healthcare communications?
Is behaviour change not the same as behavioural science?
There is a lot of talk about the need for behaviour change in the bio-pharma sector. We should all be aiming for behaviour change to improve the health of patients, enhance the adoption of new medicines in an appropriate manner and ensure that the right medicines get to the right patients at the right time. But this should be more than a fad or a gimmick.
True behaviour change requires the real-world application of behavioural science.
Ultimately, the key to any process is knowing what we want to achieve, so defining the behaviour change we need or want to see is the first thing to identify in any approach.
What is behavioural science?
Behavioural science is the study of human behaviour through systematic experimentation and observation, incorporating multiple fields of study that look at when, why and how people (and groups) behave and make decisions. This is achieved by examining the impact of factors such as conscious thoughts, motivation, social influences, contextual effects and habits. Several disciplines fall under the broad label of behavioural science, including anthropology, behavioural economics and cognitive psychology. We, in particular, are interested in the psychological aspects of behavioural science.
Behaviour is a major driver of global health problems, from substance misuse to poor diet and lack of exercise. Changing these behaviours has long been a hot topic for those in the business of improving health outcomes – and some of the most successful public health interventions have drawn from different elements of behavioural science. In recent years we’ve seen reluctant schoolchildren learning to love fruit and vegetables, smokers finally kicking the habit and healthy people lining up for a vaccine shot, all thanks to strategies built around established behavioural theory.
Behavioural science takes you beyond traditional approaches to communications
All this is nothing new, you might say – after all, the idea of taking insights research and working out what the customers want and need is the essence of marketing! But while this is still true, the healthcare sector has moved on immensely in the last few decades with multiple stakeholders (especially patients) having more say in therapies. So, while the scientific innovation in terms of development of novel therapies and approaches to diseases continues unabated, the way pharma talks to its stakeholders has changed little in that time. Behavioural science takes you beyond traditional approaches to communications and will identify the best interventions to use, leading to clear behavioural change techniques that are proven to bring about more success in changing that all-important behaviour.
The theories
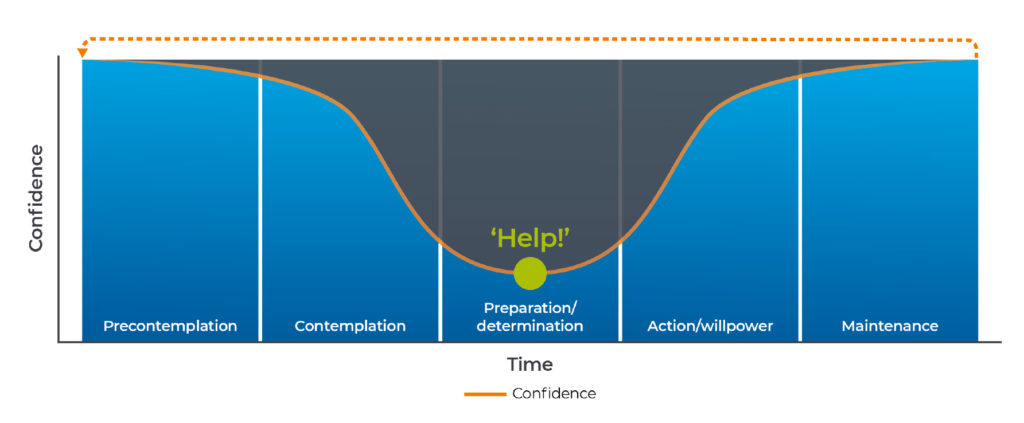
Figure 1. How confidence in behaviour varies in stages of change
Alpharmaxim formulated this model while working on a number of pre-launch assets, when it became clear that the need to overcome barriers went beyond “just communicating the efficacy and safety”. We coined the term Belief Continuum® around 2007 and were granted a trademark and copyright in 2016.
The science of behaviours has continued to move forward, leading to the development of a framework called the Behaviour Change Wheel² This framework combines aspects of many older theories and gives us a structural basis for deeper understanding of behaviours, along with the barriers that might be preventing those behaviours from changing.
A well-known component of this framework is the COM-B model (Figure 2) – this is based on the idea that in order to carry out a behaviour, an individual must have the Capability, the Opportunity and the Motivation to do so.
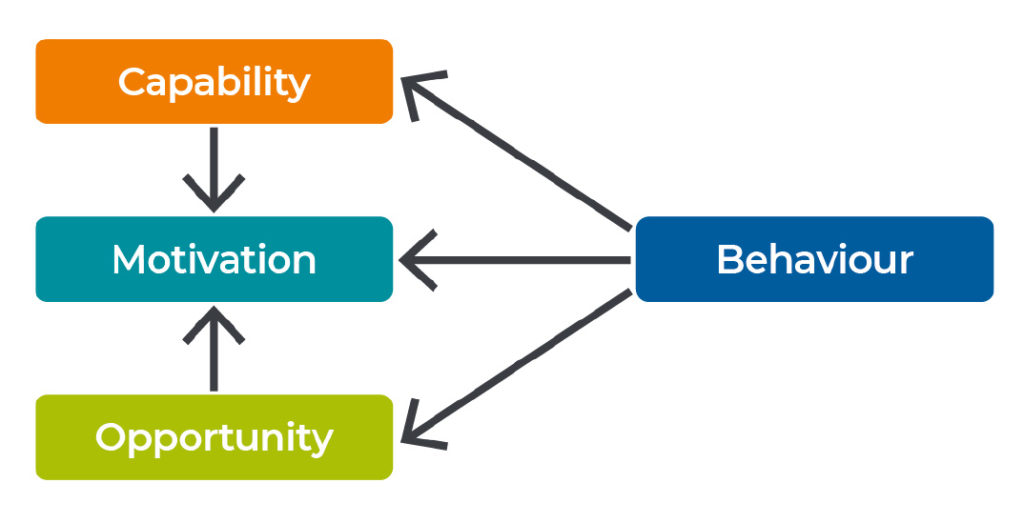
Figure 2. COM-B analysis model used to determine behavioural components3
How does this apply to communications?
Traditional approaches to developing communication strategies and tactics may involve market research telling you what is happening (but not why), and experience is used to decide how to address communications goals.
Our approach is likely to lead to improved and more objective approaches to care that benefit patients
The approach of behavioural science is to uncover the fundamental drivers of existing behaviour and the barriers to change. The most appropriate and effective tactical interventions for these barriers to change are defined, leveraging but not relying on experience alone. This takes out the guesswork and subjective bias of traditional methods and uses validated scientific approaches to clearly define what works and why. This means that a communications plan is based in validated science and is likely to be more accurate, impactful, effective and valuable. Most importantly, our approach is likely to lead to improved and more objective approaches to care that benefit patients (Figure 3). Another benefit of this approach is that it is easier to track the return on investment delivered by your updated communications; something that is of great value in these hard-pressed times.
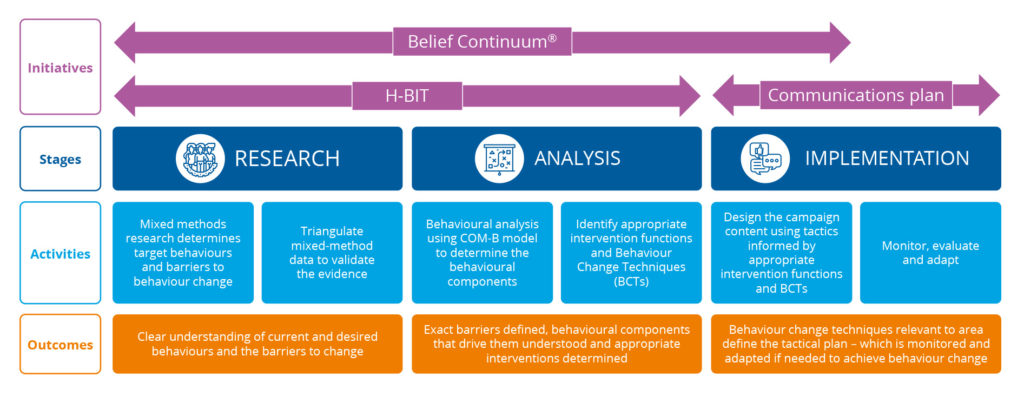
Figure 3. Behaviour change using behavioural science.
An overview of Alpharmaxim’s proprietary, scientifically validated process to drive behaviour change.
Why is behavioural science important to communications in pharma?
If uninitiated bio-pharma companies stick to their traditional approaches and keep saying the same things in the same way through the same channels, the financial backers, regulatory agencies, prescribing clinicians, and patients and their families or carers are going to stop listening. Which will mean that important new messaging fails to get through and important medical advances may be delayed or even lost.
With such huge investment and groundbreaking science occurring in all areas of medicine (but especially in rare diseases and gene therapies) and with increasing pressures to demonstrate value, it follows that the communications need to be planned with this in mind to reach all the stakeholders and communicate in the most effective way possible about the things that matter to them.
Is this approach in line with the necessary compliance and governance policies?
There is no witchcraft involved. This is not about ‘persuading people’ to do things they would otherwise not. This is a science based on experimentation. The key focus is to enable the right choices at the right time.
How can we apply behavioural science in our communications?
Alpharmaxim have developed the Healthcare Behavioural Insights Tool (H-BIT) in partnership with Aston University School of Psychology. This is a proprietary tool that facilitates the practical and rapid application of the validated approaches of behavioural science to give direction to communications planning.
Our initial work to validate the H-BIT was undertaken in neurodegenerative diseases (NDD), such as Parkinson’s and Alzheimer’s. These conditions were chosen because of their high prevalence and high unmet need. We intend to target other disease areas in the future.
Talk to us about our practical approach that utilises a validated Healthcare Behavioural Insights Tool (H-BIT) to identify and address critical barriers to change
References
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol 1983;51(3):390–395
- Michie S, Atkins L, West R. The Behaviour Change Wheel: a guide to designing interventions. Great Britain: Silverback Publishing; 2014
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 2011;6:42
