
It’s time for behavioural science to take centre stage in healthcare communications
Dan Parkinson, Principal Copywriter at Alpharmaxim Healthcare Communications
In 1977 The Jam sang, ‘this is the modern world’. It was a time of change, towards the back end of a somewhat turbulent decade when cultural sands were shifting. Today, we live in a world almost unrecognisable to the one they inhabited, a world that continues to change and evolve.
Progress brings new challenges, new ideas, new solutions. And healthcare certainly faces challenges – although not all of them are new. Here in the UK, we are constantly reminded that our National Health Service is ‘broken’ and struggling to meet ever-increasing demands. Meanwhile health organisations all around the world are trying to figure out how to deal with limited resources and ageing populations living with a variety of complex health conditions.
Help is needed. And it might be time for behavioural science to play a bigger part than ever before.
Breaking down barriers
Behaviour is a major driver of global health problems, from substance misuse to poor diet and lack of exercise. Changing these behaviours has long been a hot topic for those in the business of improving health outcomes – and some of the most successful public health interventions have drawn from different elements of behavioural science. In recent years we’ve seen reluctant schoolchildren learning to love fruit and vegetables, smokers finally kicking the habit and healthy people lining up for a vaccine shot, all thanks to strategies built around established behavioural theory.
This sort of thinking can be applied to pharma too. But with an abundance of research and different models available, it’s difficult to know quite where to start. When it comes to prescribing physicians, for example, what are the barriers that might prevent them from taking up a new medicine or solution in a given disease area? How can we help them, and their peers, to make optimal choices so they can improve patient outcomes? And what about patients themselves, what might be holding them back? It’s an area of great interest to us as an agency, and we know that the answers may not be what first comes to mind.
From our own experience of working with pharma clients, we know that some have encountered resistance to the adoption of new treatments that have real potential to enhance quality of life. This resistance can be on the part of patients, or physicians, or both – and the underlying reasons are often complex. As we’ve come to work in rare and hard-to-treat diseases, where effective new medicines don’t come along too often, we’ve seen that ingrained habits, limited experience and fear of change can prove significant hurdles to get over – even when the standard treatment method is an unpleasant one for the patient.
Every case is different though, and it’s important to make strategic behaviour change decisions based on solid evidence. But what if we could generate our own evidence, tailored to a specific disease area? What if we had a reliable way of making predictions about how audience segments might respond to different behaviour change interventions, so we could devise customised communications approaches? What would that look like, and how could we get there? These are just a few of the questions we’re currently asking ourselves, and we’re working behind the scenes to come up with the answers.
Beyond belief: putting theory into practice
The Transtheoretical Model,1 aka ‘the stages of change’, was first developed in the late 1970s, around the time when the aforementioned musicians were riding the waves of cultural change in the UK. Whether Prochaska and DiClemente were Jam fans is hard to say, but you could argue their legacy has endured equally well. Their five stages of change have influenced countless health behaviour change initiatives, notably in the design of phased interventions for smoking cessation. And it’s a model that has previously inspired our own behaviour change efforts.
Our tried-and-tested in-house approach to communications planning, the Belief Continuum®, is a process that aims to uncover the beliefs that underpin certain behaviours and work out what needs to be communicated at each stage (Figure 1) in order to change those beliefs. The concept is based on the stages of change model, but with the added layer of a series of incremental nudges to rebuild beliefs that support desired behaviours.
The Belief Continuum® approach has already helped pharma companies to clearly define narratives that can help to shift beliefs about their products and encourage both patients and HCPs to make positive changes. But we want to go further still. To really get under the skin of what drives behaviour, and go beyond targeted messaging to reach new levels of insight and understanding.
Figure 1: How confidence in behaviour varies in stages of change
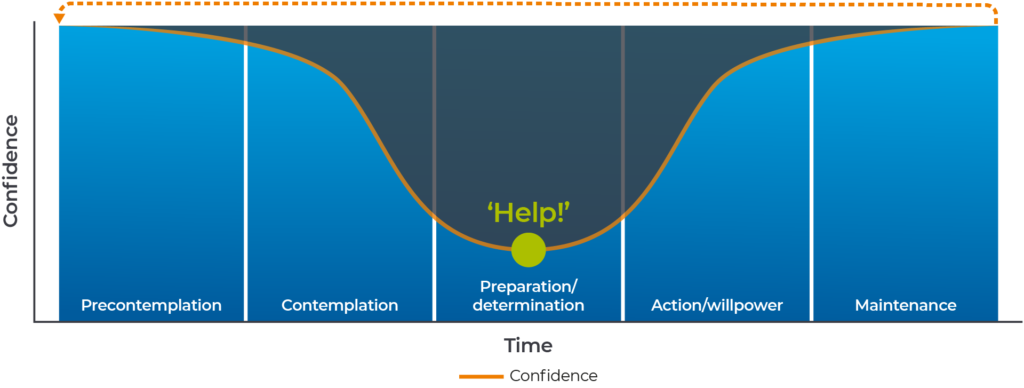
NB: The stages of change are not linear, and an individual may go back and forth through the stages during the course of the Belief Continuum®. As new health recommendations emerge the process may start again, going from stage five back to stage one.
A framework to build upon
The stages of change model is certainly useful in many contexts, but there are newer, more robust frameworks that give us freedom to explore and evaluate different interventions. The Behaviour Change Wheel,2 for example, combines aspects of many older theories and gives us a structural basis for deeper understanding of behaviours, along with the barriers that might be preventing them.
A well-known component of this framework is COM-B (Figure 2) – this is based on the idea that in order to carry out a behaviour an individual must have the Capability, the Opportunity and the Motivation to do so. A physician might be aware of a new treatment, and the unmet need it seeks to address, but they may not have access to the right resources. Perhaps they are not being encouraged to change behaviour by their peers, or the system they are working in. Maybe their motivation is reduced because the old way of doing things helped their patients to manage symptoms reasonably effectively, so they see no reason to change. But what if the new way can genuinely make a difference to care standards and quality of life? To get results, communications plans need to consider both motivation and opportunity, not just capability. It all starts with identifying and evaluating the most influential factors and the barriers to change.
Figure 2: The COM-B Framework2
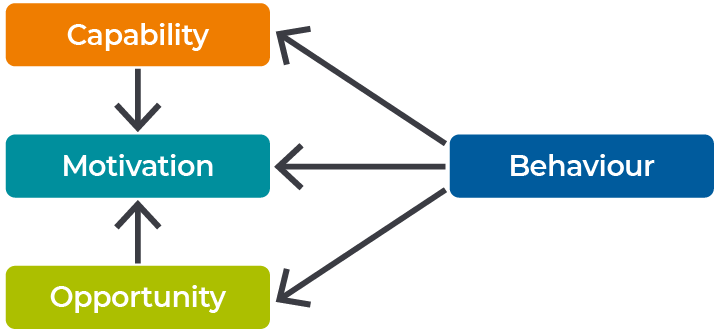
Adapted from Michie et al.2
“Understanding behavioural science won’t achieve anything without the necessary communications that follow it. Looking at the specific barriers to behaviour change can help pharmaceutical companies to prioritise and optimise their communications so that, ultimately, the right people can access the right medicines at the right time.”
Will Hind, CEO, Alpharmaxim
Behavioural science can seem like a complex subject area, but the challenges in its implementation are far outweighed by the opportunities. By applying new, simplified models and taking a targeted approach backed by evidence, we can improve the chances of potentially game-changing new practices being adopted earlier.
Creating a healthier outlook
The challenge for health communications planning is to evolve to keep up with the pace of change in the modern world – doing the same things won’t lead to different results. (And when the planner’s dream goes wrong,* that can be the bitterest pill** of all.)
At Alpharmaxim we want to contribute, by doing things differently. And by harnessing the potential of behavioural science to drive smarter, more effective communications, make better predictions, drive better decision making and help the industry to address future healthcare challenges. At a time when the health communications world is increasingly waking up to behavioural science, we believe now is the time to optimise its use, embed it more widely in our practices and help drive the changes the industry needs in the years ahead.
These are exciting times here at Alpharmaxim – look out for further updates as we move forward on our behaviour change journey.
*Sorry, one more Jam reference
**Okay two more
References
1. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol 1983;51(3):390–395
2. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 2011;6:42
